

By Dr. Fawaz al Sarayreh and Dr. Khalil Al-Salem
The lecture aims to inform medical students about Retina diseases; this includes retinal detachment, retinal vascular disorders like Central retinal artery occlusion and central retinal vein occlusion. Other medical retinal disease includes diabetic retinopathy and age-related macular degeneration.
PPT Dr. Fawaz lecture
Anatomy and physiology :
Retinal disease caused by diabetes (Diabetic Retinopathy)
People with diabetes can lose vision from macular edema, macular ischemia, vitreous hemorrhage, and tractional retinal detachment. The ophthalmologist has several tasks: 1- confirm the diagnosis; 2- classify its severity and monitor accordingly; 3- offer advice; apply retinal laser as required; 4- treat associated eye disease such as cataract.
Classification of diabetic retinopathy (مهم جدا و مطلوب)
Non Proliferative diabetic retinopathy
There are three stages of diabetic retinopathy; the first is Mild non-proliferative diabetic retinopathy (NPDR), where At least one microaneurysm is present. second stage is Moderate non-proliferative diabetic retinopathy, intraretinal haemorrhages or microaneurysms and/or cotton-wool spots, venous beading, intraretinal microvascular abnormalities (IRMA) carecterises this stage if retinal disease. Severe non-proliferative diabetic retinopathy relies on the 4–2-1 rule, which requires one of the following:
- Intraretinal hemorrhages or microaneurysms in four quadrants.
- Venous beading ≥ ETDRS photograph 6a in two quadrants.
- IRMA ( intra-retinal arterial malformation) ≥ ETDRS photograph 8a in one quadrant.
Treatment is advised if there is clinically significant macular oedema (CSMO) comprising at least one of the following:
1- Thickening of the retina within 500 μm of the fovea.
2- presence of Hard exudates located within 500 μm of the fovea with adjacent retinal thickening.
3- Retinal thickening at least one disc area in size, part of which is located within one disc diameter of the fovea.
It is essential to ask about the duration and type of diabetes, blood sugar control, smoking, and associated disease, especially hypertension and renal disease. Identify the clinicians monitoring the patient’s diabetes.
An examination should be targeted towards the presence of iris neovascularization (NVI). If the patient has Rubeosis iridis, it is important to check the intraocular pressure. Most of the time, the IOP is elevated due to the presence of secondary closed-angle glaucoma. Gonioscopy is performed to check for angle neovascularization (NVA). Perform careful fundus examination looking for atypical features. Exclude associated disease, especially posterior subcapsular cataracts.

Proliferative diabetic retinopathy:
Clinical features:
Symptoms: progressive loss of vision, particularly in those who are not properly followed or treated.
Signs: the presence of fine to severe loops of new vessels that may grow on the optic disc(neovascularization of the disc (NVD)) or neo-vessels elsewhere (NVE). PDR can affect the iris and angle as well. Neovascularization of the iris (NVI) in the anterior segment, the angle (NVA). Neovessels of the iris may cause occlusion of the angle and may lead to closed-angle glaucoma. Neovessels may leak and result in retinal edema, or it may bleed, causing vitreous hemorrhage. Opaque fibrovascular proliferation tissue often appears on the internal limiting membrane (adjacent to the new vessels) and becomes adherent to the vitreous. Contraction of this fibrovascular tissue may lead to:
1- Distortion or dragging of the macula
2- tractional retinal detachment
3- Avulsion of retinal vessels and vitreous hemorrhages
Risk factors:
Duration of the diabetes, 30-34 years of diabetes increase the risk of retinopathy by 65%
Overt albuminuria
High level of blood total cholesterol and LDL
Others: race, cigarette smoking, alcohol
Management of retinal disease caused by DR:
Strict blood glucose, blood pressure and cholesterol control.
Photocoagulation for clinically significant macular edema prior to scatter (panretinal) photocoagulation (PRP).
Consider PRP in severe proliferative diabetic retinopathy. Consider additional PRP if incomplete regression is observed, increasing of the extent of vitreous hemorrhage or worsening of overall vitreoretinal condition.
Vitrectomy.
Experimental treatments; Depo steroid injection for diabetic macular edema, systemic protein kinase-C inhibitor and aldolase reductase inhibitor.
Differential diagnosis of Diabetic Retinopathy
Differential diagnosis of Nonproliferative diabetic retinopathy includes central or branch retinal vein occlusion; ocular ischaemic syndrome; hypertensive retinopathy; radiation retinopathy; leukaemia; anaemia; HIV microangiopathy.
Differential diagnosis of Proliferative diabetic retinopathy includes vascular obstruction; sickle cell retinopathy; ocular ischaemic syndrome; sarcoidosis; Eales’ disease; tuberculosis; embolization from intravenous drug use.
Complications of diabetic retinal disease
Vitreous hemorrhage.
Treat mild vitreous hemorrhage as high-risk PDR. If the hemorrhage is dense enough to obscure the fundal view, perform B-scan ultrasound to exclude retinal detachment. Review monthly to monitor for iris new vessels or raised IOP. Apply PRP as hemorrhage clears and the view improves. Arrange vitreoretinal review if the hemorrhage persists for 1 month (type 1 diabetes), or 3–4 months (type 2). Consider early referral if the other eye has poor acuity.
Tractional retinal detachment.
If tractional retinal detachment threatens the macula, arrange vitreoretinal review. If not, review 2–3 monthly depending on the retinopathy severity.
Maculopathy.
1. Not clinically significant: review in 4–6 months.
2. Clinically significant macular oedema: perform fluorescein angiography unless there is an isolated circinate, and treat as per ETDRS:
a. Laser treatment for the macula, Avoid laser treatment to the edge of, or within, the foveal avascular zone (FAZ).
b. Give intravitreal steroids’ of anti-VEGF to shrink the thickness of the macula
Consider earlier review for all categories if there is poor diabetic or blood pressure control, or recent marked improvement in diabetic control (can transiently worsen retinopathy).
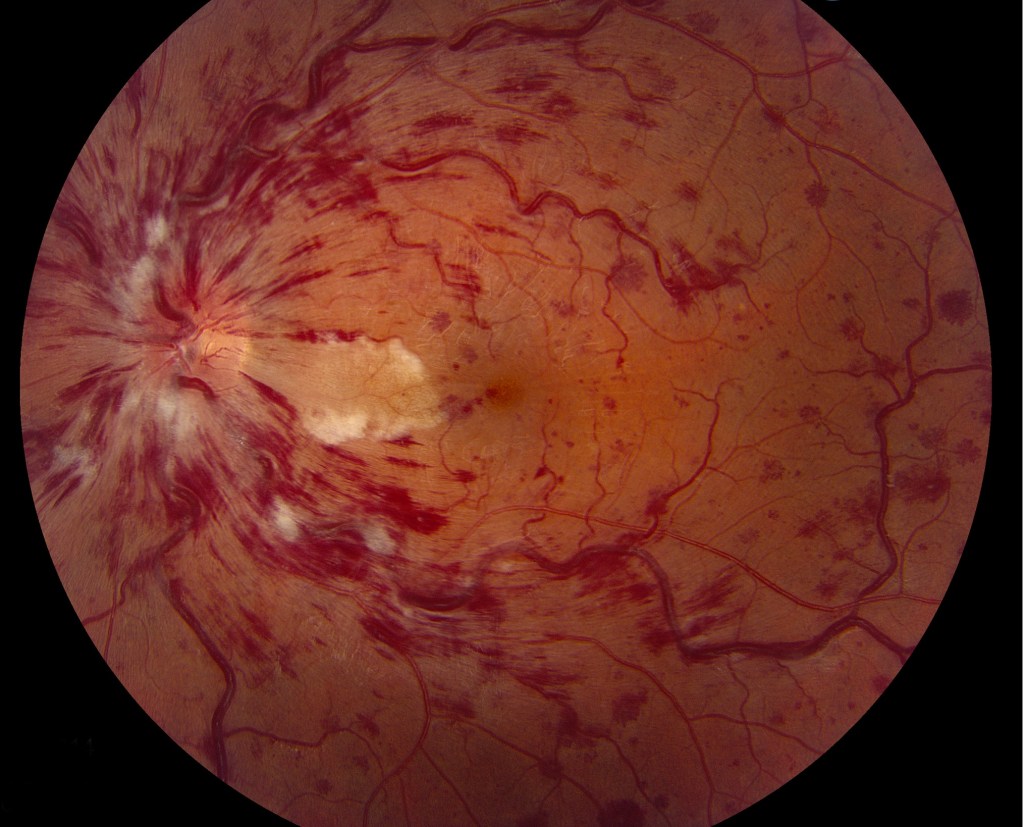
Examples of Diabetic retinopathy :


Dr. Fawaz Al Saryreh lecture, retinal vascular diseases
PPt for Dr. Fawaz
Central retinal vein occlusion:
Central retinal vein occlusion (CRVO) typically occurs in patients over 45 years secondary to retinal vein thrombosis. Risk factors include diabetes, hypertension, hyperlipidaemia, and glaucoma. CRVO in those aged less than 45 years may suggest a clotting disorder. It is important to start those patients on anti coagulants.
Clinical features of retinal disease caused by CRVO
Painless visual loss in one eye. loss of vision can vary between patients according to the severity of macular ischemia
Signs include: retinal hemorrhages in four quadrants; dilated tortuous retinal veins; optic disc swelling; macular edema; cotton-wool spots; neovascularization of the iris, angle, retina, or disc.
Classification of CRVO retinal disease:
Classification is based on the macular involvement and severity of Ischemia, we have
■ Nonischaemic CRVO
■ Ischaemic CRVO
1. Clinical examination: presence of Relative afferent pupillary defect (RAPD), Visual acuity better than 6/60, multiple cotton wool spots, dense mid-retinal hemorrhages, ‘blood and thunder fundus’.
2. Fluorescein angiogram: more than 10 disc areas of ischaemia. History and examination Ask about glaucoma, systemic hypertension, raised lipids, diabetes or symptoms of diabetes (polyuria, polydipsia, weight loss).
If the patient is younger than 45 years ask about thrombophilia: family history of thromboses aged <45 years; deep vein thrombosis; pulmonary emboli; thromboses in unusual sites, e.g. axillary vein; multiple miscarriages. Examine specifically for new vessels in the angle (undilated gonioscopy), iris, and optic nerve/retina. Examine both eyes for features of glaucoma.
Differential diagnosis of retinal disease caused by CRVO
Consider ocular ischaemic syndrome; diabetic retinopathy; optic disc swelling for other reasons; and radiation retinopathy.
Investigations and work up of CRVO
Check blood pressure, Fasting blood sugar, ESR, lipids (thyroid function if abnormal), plasma protein electrophoresis, and thrombophilia screen if suspicious. Arrange macular OCT (optical coherence topography).
Treatment of CRAO Retinal disease
Start with low-dose antiplatelets and discontinuation of oral contraceptives. Treat glaucoma, and Consider macular grid laser for patients <50 years with macular oedema and no angiographic evidence of macular ischaemia. Hypertension is important to be controled in this disease, as it causes recurrence of CRVO
Branch Retinal Vein Occlusion
Background Branch retinal vein occlusion (BRVO) occurs 2–3 times more common than central retinal vein occlusion (CRVO) but has similar risk factors. The major sequelae are macular edema and vitreous hemorrhage from the disc due to retinal new vessels. BRVO affecting the entire superior or inferior retina (hemi-central vein occlusion) has a higher risk of rubeosis and disc new vessels. Symptoms Usually painless loss of vision in one eye but may be asymptomatic. Rubeosis is less common; macular edema, disc, and retinal new vessels, more so.
Classification of BRVO retinal disease
■ Ischaemic: >5 disc areas of ischaemia on fluorescein angiography.
■ Nonischaemic: <5 disc areas on angiography.
History and examination and treatment similar to CRVO

Central Retinal Artery Occlusion
Symptoms Sudden, painless, unilateral, often severe visual loss.
Retinal signs include retinal opacification, whitening, edema; a cherry-red spot at the macula; RAPD; with possible cilioretinal artery sparing.
History and examination of retinal artery occlusion

It is important to ask about transient ischaemic attacks, cerebrovascular accidents, symptoms of giant cell arteritis, or amaurosis fugax (retinal emboli causing transient uniocular visual obscuration lasting a few minutes).
Auscultate the carotids for bruits using the stethoscope bell, check heart sounds for a valvular murmur, and radial pulse for atrial fibrillation. Look for intra-arteriolar calcific, cholesterol, or fibrino-platelet emboli.
Differential diagnosis of CRAO retinal disease :
Differential diagnosis of a cherry-red spot at the macula
1- Metabolic Storage Diseases: Tay–Sachs disease
2- Farber diseaseGM1 and GM2 gangliosidoses
3- Metachromatic leukodystrophy
4- Niemann–Pick disease
5- Sandhoff disease
6- SialidosisCongenital
Developmental diseases (e.g., Leber’s congenital amaurosis)
Hereditary/ Familial: Pantothenate kinase-associated neurodegeneration
Vascular (e.g., central retinal artery occlusion)
Drugs: Quinine toxicity, Dapsone toxicity
Poisoning: Carbon monoxideMethanol
Also, consider giant cell arteritis, intraocular gentamicin toxicity, and acute ophthalmic artery occlusion.
Investigations: Arrange BP; urgent ESR and CRP; blood sugar; FBC; lipids; ANA, rheumatoid factor, serum protein, and hemoglobin electrophoresis; thrombophilia screen if suggested by history; carotid artery Doppler; fluorescein angiogram and cardiac examination for embolic source. Investigations other than basic blood tests may be best undertaken by a physician.
Treatment: If symptoms suggest occlusion for <24 hours duration, attempt to dislodge an embolus by:
1- Firm ocular massage through closed eyelids for 15 minutes.
2- Stat crushed acetazolamide 500 mg p.o.,
3- Offer anterior chamber paracentesis but explain that results are variable. If performed, prescribe G. chloramphenicol q.d.s. one week.
Follow–up: Review initially in 2–4 weeks. Examine for iris neovascularization. Perform or review investigations and liaise with relevant clinicians. Advise immediate ophthalmic review if visual obscuration occurs in either eye. Local policies for carotid endarterectomy vary and depend on the degree of carotid occlusion, so discuss with a vascular surgeon.
Branch Retinal Artery Occlusion
Symptoms: Unilateral, painless, sudden, visual field loss.
Signs: Retinal swelling similar to central retinal artery occlusion (CRAO, previous page), except for branch distribution. Emboli may be present.
Classification:
■ Single episode.
■ Multiple episodes: consider systemic disease and urgent medical review.
History, examination, investigations See CRAO, above. Cilioretinal occlusion may occur in the presence of central retinal vein occlusion and is commonly missed. Exclude giant cell arteritis.
Treatment: No therapy is of proven value.
Follow–up: Initiate medical follow-up as indicated by the investigations. Evaluate for recurrences or new disease in 3–6 months. About 80% of symptomatic cases achieve VA of 6/12 or better.