

written By Prof. Khalil Al-Salem M.D FRCS, FICO
Neuro-ophthalmology II is a dedicated lecture designed for medical students at Mutah University, covering various topics such as Anisocoria, Adie’s tonic pupil, Horner’s syndrome, transient visual loss, and Visual field defect.
Anisocoria, and Neuro-ophthalmology: difference in the pupillary size
When it comes to Anisocoria in the field of Neuro-ophthalmology, it’s essential to understand the difference in pupillary size. Begin by asking who first noticed the anisocoria and attempt to establish its duration. It can be helpful to review old photos, and magnification may be required to assess pupil size. Additionally, it’s crucial to exclude a history of neck or chest surgery or injury, limb weakness, difficulty focusing, diplopia, and ptosis.
Neuro-ophthalmology lecture
Neuro-ophthalmology, Examination of the pupil:
In the examination of the pupil in the field of Neuro-ophthalmology, it’s essential to identify which pupil is abnormal. This can be accomplished by examining first in the dark and then in the light. Greater anisocoria in the dark indicates impaired dilatation (sympathetic dysfunction), while greater anisocoria in the light indicates impaired constriction (parasympathetic dysfunction). It’s worth noting that physiological anisocoria is usually ≤2 mm, and the difference remains the same at all light levels. Be sure to examine the pupils and the iris on the slit lamp for a comprehensive evaluation.
Differential diagnosis of abnormally large pupil:
Dilating drops, like atropine, tropicamide and cyclopentolate.
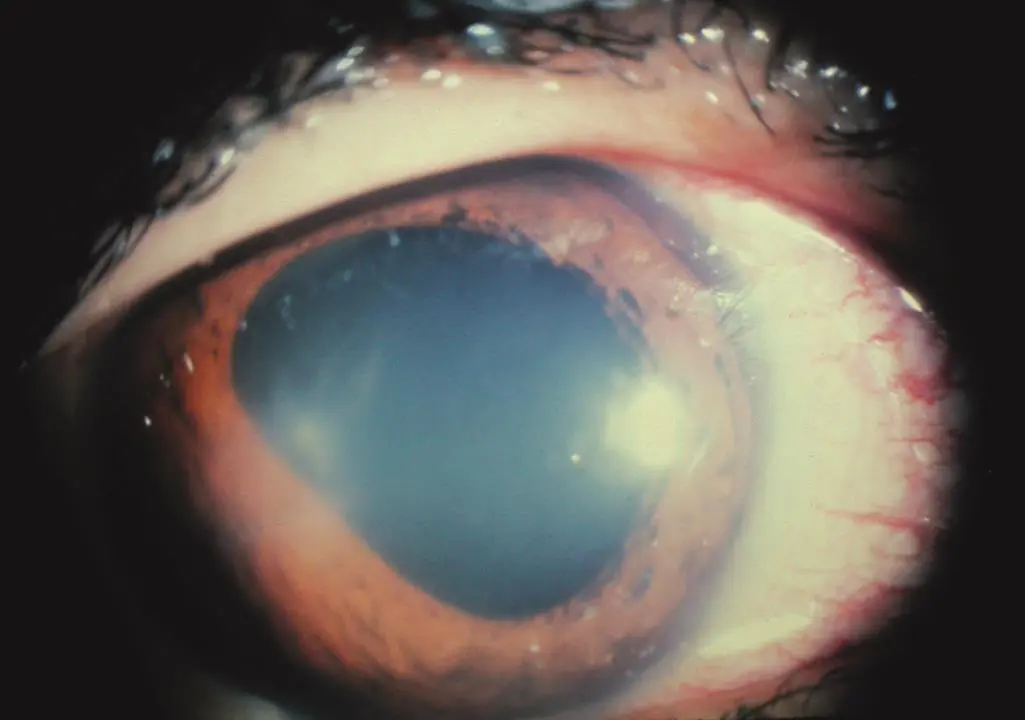
Traumatic mydriasis, dilatation of the pupil secondary to blunt trauma
Iris rubeosis, presence of neo-vessels, in the iris secondary to ischemia which is caused by vascular occlusion or severe chronic inflammation.
Urrets-Zavalia syndrome (iris atrophy following corneal graft),
physiological anisocoria, witch is the most common cause.
Neuro-ophthalmology and Adie’s tonic pupil
Adie’s tonic pupil, also known as the Holmes-Adie pupil, is characterized by the presumed post-viral denervation of the sphincter pupillae and ciliary muscle, resulting in anisocoria and difficulty focusing. As reinnervation occurs, accommodation typically recovers within a few weeks, but it’s worth noting that the sphincter pupillae becomes partially innervated by lens fibers during this process.
Adie’s tonic pupil signs
Signs that follow include light-near dissociation, characterized by slow or absent constriction to light but a prompt constriction on attempted near vision. Additionally, a segmental sphincter palsy observed during a slit lamp examination gives rise to the so-called vermiform movements of the iris, along with absent limb reflexes.
The feature that sets Adie’s tonic pupil apart is its slow dilation following accommodation, often referred to as tonic constriction, which differentiates it from Argyll Robertson pupils. It’s crucial to exclude ptosis and diplopia, as they might indicate a 3rd nerve palsy. Notably, while normal pupils typically do not constrict to G. pilocarpine 0.125%, Adie’s tonic pupil does, a phenomenon known as denervation hypersensitivity. However, this test has only moderate specificity, as preganglionic lesions can exhibit a similar response. In most cases, further investigations are not necessary. It’s advisable to arrange routine referral to a neuro-ophthalmologist, and long-term follow-up is usually unnecessary. Adie’s tonic pupil often manifests bilaterally but with an asymmetric presentation, and over time, the affected pupils tend to become smaller.
Regarding the differential diagnosis of Adie’s tonic pupil, one should consider the possibility of an abnormally small pupil. This can be associated with conditions like Horner’s syndrome (as discussed below), the use of pilocarpine drops, uveitis leading to posterior synechiae, chronic unilateral aphakia, and physiological anisocoria.
Horner’s syndrome ( Neuro-ophthalmology point of view)
■ Horner’s syndrome: Sympathetic denervation produces miosis and mild ptosis. It may be preganglionic or postganglionic.
Preganglionic Horner’s syndrome
Preganglionic (central) causes include lung (Pancoast tumor) and breast malignancy, sympathetic chain schwannoma, and cervical spine damage (e.g. C8 or T1 disc prolapse).
postganglionic Horner’s syndrome
Postganglionic causes include internal carotid dissection, neck tumours, cavernous sinus disease (especially if 6th nerve palsy coexists), and cluster headache.
Horner’s syndrome diagnosis:
The diagnosis of Horner’s syndrome is Confirmed by Continued pupil Constriction despite G. Cocaine 4% (delay further pharmacological testing for 2 days after cocaine testing). Preganglionic causes produce ipsilateral anhidrosis of the face (ptosis, miosis, anhidrosis) and the pupil dilates with G. hydroxyamphetamine 1% (no effect if postganglionic).
Neuro-ophthalmology investigations in Horner’s syndrome
Investigations: depend on the likely cause, but if painful request urgent T2 weighted MRI axial scans to exclude carotid dissection. This is associated with a high risk of embolic stroke within 10 days and anticoagulation is indicated.
Congenital preganglionic Horner’s syndrome typically has iris heterochromia and is seen on old photographs. Acquired childhood cases require investigation to exclude neoplasia, particularlarly cervicothoracic neuroblastoma, though most are benign.
Neuro-ophthamology causes of Transient Visual Loss
History Ask about: duration; whether one or both eyes are affected; total blackness (arterial occlusion) or just blurred; patchy grey blobs (spasm of choroidal vessels); cardiovascular risk factors; TIAs or strokes; known carotid disease; headache; migrainous aura; dizziness, hearing, or speech problems; loss of balance; haloes; eye pain; abnormal clotting (DVTs); scalp tenderness; jaw claudication (over 50 years).
Specific precipitating factors may suggest the diagnosis:
1- Bright light: chronic retinal ischaemia due to carotid insufficiency.
2- Eye movements: space-occupying orbital lesions or an optic nerve tumour.
3- Prolonged reading or evening onset: intermittent angle-closure glaucoma.
4- Exercise: pigment dispersion syndrome.
5- Standing up: usually indicates reduced perfusion pressure including postural hypotension, carotid insufficiency, and giant cell arteritis (precedes nerve infarction). Papilloedema may produce brief monocular or bilateral obscurations with either standing up or stooping down.
Neuro-ophthalmology Examination related Transient loss of vision:
Check BP in both arms (sitting and standing if appropriate); radial pulse; cardiac and carotid auscultation; temporal artery palpation (in patients over 50 years); VA; confrontation visual fields; colour vision; RAPD; corneal clarity (oedema or endothelial pigment); iris rubeosis; gonioscopy (is angle closeable?); IOP; dilated fundoscopy (especially retinal vessels for emboli, venous dilation, retinal haemorrhages and optic disc for swelling); assess central retinal artery perfusion pressure; other tests as indicated.
Differential diagnosis of transient loss of vision
■ The following are the more common or serious causes:
1. Carotid or cardiac emboli
2. Carotid dissection: may have neck pain and Horner’s syndrome ( the patient has sudden severe pain in the head the neck).
3. Migraine: usually hemianopia, positive features, with zigzags typical ( very common cause in young females).
4. Giant cell arteritis
5. Vertebrobasilar insufficiency
6. Intermittent angle-closure glaucoma
7. Occipital embolus: may cause hemianopia loss or transient blindness.
8. Retinal arterial embolus: typically, a curtain descent to a blackout.
9. Retinal vasospasm: more likely a whiteout, and very related to Migraine headache.
10. Choroidal vasospasm: vision disappears in patches.
11. Cardiac dysrhythmia: blindness may precede loss of consciousness or occur in isolation.
12. Occipital epilepsy: usually hemianopia with positive symptoms such as coloured circles.
Management of transient visual loss
Management Investigation and treatment depends on the likely cause. In the case of transient monocular blindness, emboli usually arise from the aorta, carotids, or heart valves. Most commonly, they are cholesterol, platelet-fibrin, or calcific, but septic, amniotic fluid, air, fat or talc (i.v. drug users) may rarely occur in specific situations. If likely, start oral aspirin 75 mg o.d. Don’t forget to refer your patient to the cardiologist
Neuro-ophthalmology and Visual field defect
The accurate delineation of visual field defects is critical to the diagnosis of visual pathway lesions. Visual field defects are frequently asymptomatic and may be detected on routine screening (usually by an optometrist) or when field tests are preformed for some other reason. An awareness of the various artefactually produced field defects is important.
Symptoms Patients are less likely to notice field defects from optic nerve or visual pathway lesions if these spare the central field. Retinal lesions often produce positive scotomas with patients aware of photopsia within the visual field defect.
History: ِِAsk when and how the field defect was first noticed. Sudden onset or gradual? Any recovery? Ask about cardiovascular risk factors, photopsia, pain, headache and other neurological symptoms, and symptoms of pituitary disease (amenorrhoea, hypothyroidism, loss of libido, headache, and acromegaly).
Neuro-ophthalmology Examination in Visual field defect :
Check Blood pressure, cranial nerves, visual acuity, color vision, RAPD, formal fields, eye movements, intra-ocular pressure, assess angle, and dilated fundoscopy. Exclude ptosis, and disc cupping, pallor, or swelling. Many Visual Field Defects are relative (partial), and not absolute (complete).
Differential diagnosis Visual field defect may be caused by retinal pathology (e.g. retinal detachment or vein occlusion).
A cataract may cause a globally decreased field but not focal defects. A homonymous hemianopia should not cause a decreased visual acuity. Glaucoma can cause a range of visual field defect but confirm that the field defect corresponds to the sectoral neuro-retinal rim thinning; color vision is relatively well preserved until late in the disease, unlike optic nerve disease.
Types of visual field defects in Neuro-ophthalmology
First , Left homonymous hemianopia :
Consider a right post chiasmal lesion such as occipital lobe CVA or tumor. The more congruous the field defect, the nearer to the occipital lobe, but a large lesion affecting both temporal and parietal lobes (the entire optic radiation) could also cause this.
Second, Left superior homonymous quadrantanopia:
Probably right inferior occipital cortex but consider right temporal lobe lesion. Inferior homonymous quadrantanopia may be caused by a parietal lobe lesion. The defect may be relative or absolute. The vertical meridian will be absolutely respected but usually not the horizontal meridian.
Third, Bitemporal superior quadrantanopia
Typically caused by pituitary tumors but will be relative; the defect will respect the vertical meridian but not the horizontal meridian.
As the defect progresses, the bitemporal hemianopia will become more complete but usually asymmetric and eventually with evidence of optic neuropathy on one or other side. A craniopharyngioma may cause a bilateral inferotemporal quadrantanopia but is more likely to give rise to a combination of the optic nerve, chiasm and tract deficits.
Fourth Complete bitemporal hemianopia:
May occur with compressive lesions of the chiasm but such a clear-cut deficit is typically only seen in cases of traumatic chiasmal transection.
Central scotoma:
The commonest cause is age-related macular degeneration. In the case of optic nerve disease, such a symmetrical picture is more likely to be toxic, nutritional, or an inherited condition. Cone dystrophy can produce a similar picture.
Superior altitudinal heminaopia
In the left eye: typically seen with non-arteritic anterior ischemic optic neuropathy but also normal pressure glaucoma (usually bilateral and with arcuate defects in the lower field also), hemicentral vein occlusion, branch retinal artery occlusion, ptosis (less severe), sector panretinal photocoagulation (PRP) laser, and inferior retinal detachment.
Concentric peripheral field loss
May be seen in retinitis pigmentosa, chronic atrophic papilloedema (e.g.idiopathic intracranial hypertension), end-stage glaucoma, PRP, central retinal artery occlusion with cilioretinal artery sparing (usually unilateral), optic neuropathies, and in vigabatrin toxicity.

| Locus of the visual pathway | Blood supply | Field defect | Typical lesions | Notes |
| Optic nerve | Ophthalmic artery | Ipsilateral monocular blindness | Optic neuritis Amaurosis fugax Optic atrophy Retrobulbar optic neuropathy Trauma | |
| Optic chiasm | Branches from: Internal carotid Posterior communicating artery Anterior cerebral artery Anterior communicating artery | Bitemporal hemianopia (central chiasm) ——————————- Ipsilateral monocular nasal hemianopia (peripheral chiasm) | (Central chiasm) Pituitary adenoma Suprasellar aneurysm ——————- Peripheral chiasm Internal carotid artery atheroma | |
| Optic tract | Middle cerebral artery (MCA) | Contralateral homonymous hemianopia | MCA Stroke | |
| Optic radiation | Middle cerebral artery (MCA) | Contralateral homonymous quadrantanopia | MCA Stroke | |
| Calcarine sulcus | Mostly by the PCA. The MCA also helps supply the anterior portion, which corresponds to the macula. | Contralateral homonymous hemianopia with macular sparing | PCA, Posterior communicating artery | |
| Occipital cortex | Mostly by the PCA. The MCA also helps supply the anterior portion, which corresponds to the macula. | Contralateral homonymous hemianopia with macular sparing | PCA, Posterior communicating artery |