

Written By Prof. Khalil Alsalem lecture given by Dr. Husam al Bana
Keratoplasty, commonly known as corneal transplantation, is one of the most important surgical procedures in ophthalmology. It is performed when the cornea becomes cloudy, scarred, thin, swollen, irregular, or structurally damaged in a way that affects vision or threatens the integrity of the eye. The cornea is the clear front window of the eye, and even small changes in its clarity or shape can cause major visual disturbance. For many patients with advanced corneal disease, keratoplasty can restore sight, relieve pain, and improve quality of life.
In the past, corneal transplantation usually meant replacing the entire thickness of the cornea. This traditional operation is called penetrating keratoplasty. Today, however, corneal surgery has become much more selective. Instead of replacing the whole cornea in every patient, surgeons can replace only the diseased layer while preserving the healthy parts of the patient’s own cornea. This has led to the development of lamellar keratoplasty, deep anterior lamellar keratoplasty, endothelial keratoplasty, and epithelial or limbal stem cell transplantation.
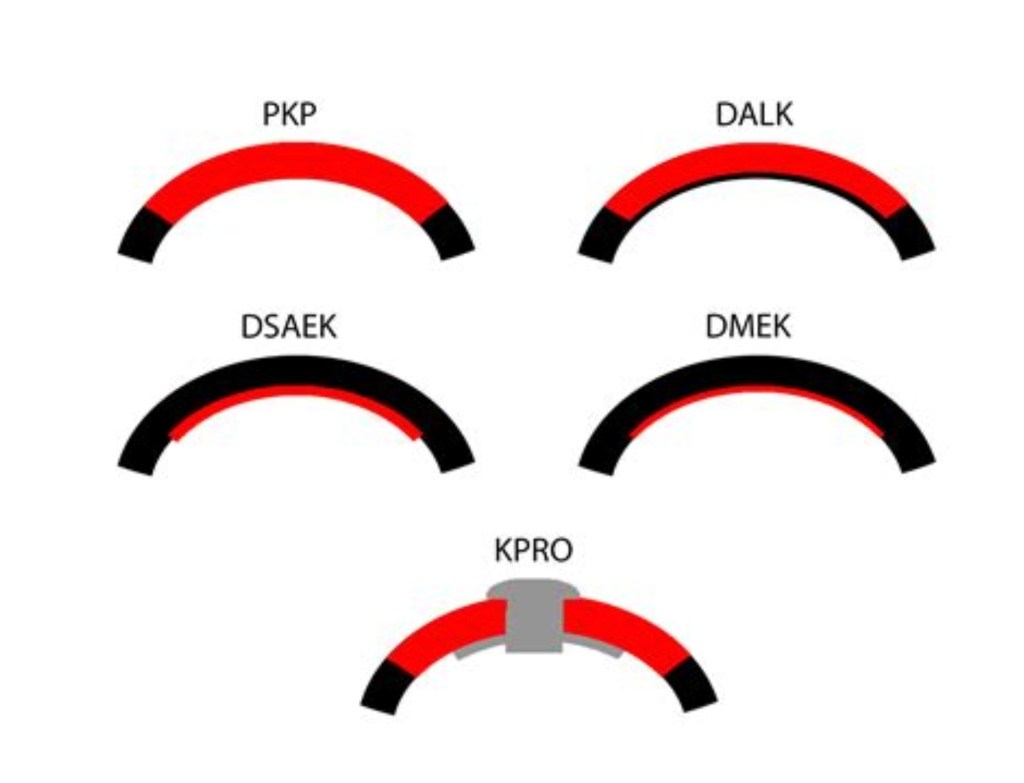
The choice of keratoplasty depends on which part of the cornea is diseased. If all layers are scarred or damaged, penetrating keratoplasty may still be required. The front and middle layers are affected but the endothelium is healthy, DALK may be preferred. If the problem lies mainly in the endothelial layer, procedures such as DSEK, DSAEK, or DMEK are usually considered. If the surface epithelium cannot regenerate properly, epithelial or limbal stem cell transplantation may be needed.
Pentrating Keratoplasty the Mother of all Keratoplasty procedures
Penetrating keratoplasty, also called PK or PKP, is the classic full-thickness corneal transplant. In this procedure, the surgeon removes the central diseased cornea through its full depth and replaces it with a full-thickness donor corneal graft. It is called “penetrating” because the operation enters the eye and creates an open-sky surgical situation.
PK has been performed for decades and remains an important operation in modern corneal surgery. It is especially useful when the disease involves several layers of the cornea at the same time. For example, a patient with a deep corneal scar, severe infection, traumatic injury, corneal perforation, or failed previous transplant may not be suitable for a partial-thickness procedure. In these cases, replacing the full corneal thickness may give the best structural and visual result.
During penetrating keratoplasty, a circular trephine is used to remove the diseased cornea. A donor cornea of a matching size is then sutured into place using very fine nylon sutures. These sutures may stay in the eye for months or even longer, depending on healing, astigmatism, and surgeon preference. Because the wound is large and circular, visual recovery after PK is usually slow. Patients may need glasses, contact lenses, or additional procedures to manage postoperative astigmatism.
The main advantage of penetrating keratoplasty is that it can treat complex corneal disease involving the full corneal thickness. It is versatile and remains essential in cases where lamellar surgery is not possible. However, PK also carries important disadvantages. Since the donor endothelium is transplanted, the patient is at risk of endothelial rejection. The eye is also structurally weaker after surgery because of the full-thickness wound. Other possible complications include infection, glaucoma, cataract, wound dehiscence, irregular astigmatism, and graft failure. PKP is defined as complete replacement of the host cornea with a full-thickness donor graft.
Deep Anterior Lamellar Keratoplasty
Deep anterior lamellar keratoplasty, usually abbreviated as DALK, is a partial-thickness corneal transplant. Unlike penetrating keratoplasty, DALK does not replace the entire cornea. Instead, it removes the diseased anterior corneal tissue, mainly the epithelium and stroma, while preserving the patient’s own Descemet membrane and endothelium.
This distinction is very important. The endothelium is the innermost corneal layer and is responsible for keeping the cornea clear by pumping fluid out of it. If the patient’s endothelium is healthy, replacing it is unnecessary and may expose the patient to avoidable rejection risk. DALK is therefore especially useful in diseases such as keratoconus, anterior stromal scars, and stromal dystrophies where the corneal shape or clarity is abnormal but the endothelial layer still functions well.
One of the best-known DALK techniques is the big-bubble method. In this method, air is injected into the corneal stroma to separate it from Descemet membrane. The surgeon then removes the diseased stromal tissue and sutures a donor graft into place. The donor tissue usually does not include endothelium. This allows the patient to keep their own endothelial cells.
DALK advantages and disadvantages
The greatest advantage of DALK is the reduced risk of endothelial rejection. Since the patient’s own endothelium remains in place, one of the most serious types of graft rejection is avoided. DALK also maintains better structural integrity than PK because the eye is not opened in the same full-thickness manner. This can be particularly valuable in younger patients with keratoconus, who may live with the graft for many decades.
However, DALK is technically demanding. The surgeon must dissect very close to Descemet membrane without perforating it. If a large perforation occurs, the procedure may need to be converted to penetrating keratoplasty. Visual outcomes after DALK can be excellent, but they may be affected by interface haze or residual stromal irregularity. Other complications include double anterior chamber, suture-related problems, infection, and postoperative astigmatism.
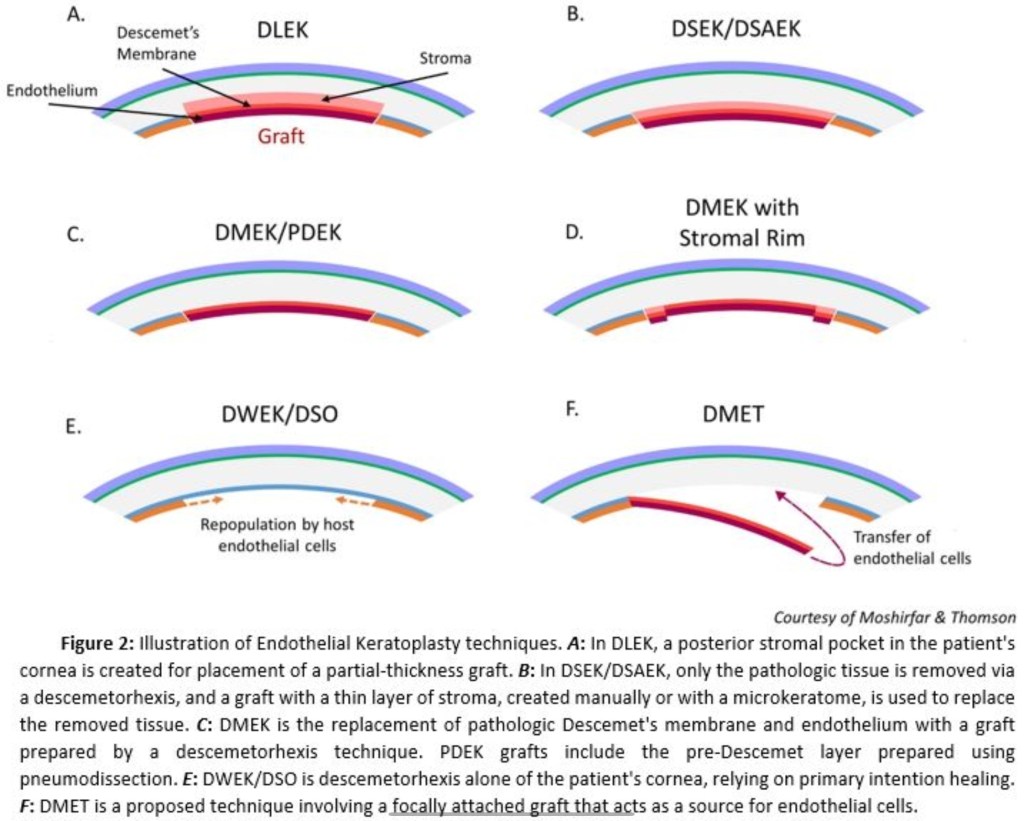
Endothelial Keratoplasty
Endothelial keratoplasty, or EK, refers to a group of procedures designed to replace the diseased endothelial layer of the cornea. This has been one of the biggest advances in corneal transplantation. Instead of removing the entire cornea, the surgeon removes the abnormal endothelium and Descemet membrane and replaces them with donor posterior corneal tissue. The goal is to restore endothelial pump function, allowing the swollen cornea to clear.
Endothelial keratoplasty is commonly used for Fuchs endothelial dystrophy, pseudophakic bullous keratopathy, aphakic bullous keratopathy, endothelial failure after eye surgery, and some failed previous corneal grafts. These conditions share a similar problem: the endothelial cells cannot maintain normal corneal hydration, so the cornea becomes swollen and cloudy.
Compared with penetrating keratoplasty, endothelial keratoplasty usually offers faster recovery, less postoperative astigmatism, fewer suture-related problems, and better preservation of eye strength. Because the surgical incision is smaller and the front corneal surface is mostly preserved, the optical result is often better and more predictable.
The main endothelial keratoplasty procedures are DSEK, DSAEK, and DMEK. They are related, but not identical. The difference lies mainly in the thickness and composition of the donor graft.
Descemet stripping endothelial keratoplasty, or DSEK
DSEK, was one of the earlier modern endothelial keratoplasty techniques. In DSEK, the patient’s diseased Descemet membrane and endothelium are stripped away and replaced with donor tissue containing endothelium, Descemet membrane, and a thin layer of posterior stroma. EyeWiki describes DSEK as replacing the patient’s Descemet membrane with a partial-thickness graft made of posterior stroma, Descemet membrane, and endothelium.
DSEK represented a major improvement over penetrating keratoplasty for endothelial disease. Because the anterior cornea is left mostly untouched, patients often recover vision faster than after PK. There is also less induced astigmatism, since the procedure does not require a full circular corneal wound with multiple sutures.
The disadvantages of DSEK are mainly related to the donor stromal layer. Because some posterior stroma is transplanted, there is an interface between donor and host tissue. This interface can sometimes limit the sharpness of vision. Patients may also develop a hyperopic shift, meaning the eye becomes slightly more farsighted after surgery.
Complications of DSEK include graft detachment, primary graft failure, endothelial cell loss, pupillary block glaucoma, interface haze, infection, and rejection. Graft detachment is one of the most recognized complications and may require an additional air or gas injection, commonly called rebubbling, to reposition the graft.
Descemet stripping automated endothelial keratoplasty, or DSAEK
DSAEK, is a refinement of DSEK. The basic surgical concept is similar, but the donor tissue is prepared using an automated microkeratome. This allows the donor graft to be cut in a more standardized and reproducible way.
DSAEK became widely used because it made endothelial keratoplasty more predictable for many surgeons. The donor graft includes endothelium, Descemet membrane, and a thin layer of posterior stroma. It is inserted into the eye through a small incision and positioned against the back surface of the patient’s cornea, usually with the help of an air bubble.
The advantages of DSAEK are similar to DSEK: faster rehabilitation than PK, reduced astigmatism, smaller incision, improved wound stability, and fewer suture-related problems. It is also generally easier to perform than DMEK, which makes it useful in complex eyes or in patients with previous ocular surgery.
The main limitation is that vision may not be quite as sharp as with DMEK, because the stromal interface can still affect optical quality. Complications include graft dislocation, endothelial cell loss, rejection, interface opacity, steroid-related glaucoma, and primary graft failure.
Descemet membrane endothelial keratoplasty, or DMEK
DMEK, is currently the most anatomically selective form of endothelial keratoplasty. In DMEK, only Descemet membrane and endothelial cells are transplanted. No donor stroma is included. Because it replaces only the diseased layer, it restores the cornea more closely to normal anatomy.
DMEK is most commonly performed for Fuchs endothelial dystrophy and other forms of isolated endothelial failure. Many corneal surgeons consider it the preferred procedure when the eye is otherwise suitable, because it can provide excellent visual quality and rapid recovery. Evidence reviews have supported DMEK as safe and effective for endothelial failure, especially in terms of visual recovery and outcomes.
The major advantage of DMEK is optical clarity. Since there is no stromal interface, the cornea can become very clear, and many patients achieve excellent visual acuity. DMEK is also associated with a low risk of immune rejection compared with older transplant techniques. A 2025 review reported that DMEK tends to provide better visual outcomes than DSAEK.
The main disadvantage is surgical difficulty. DMEK tissue is extremely thin and delicate. It can scroll, fold, or tear during preparation and insertion. The surgeon must unfold and position the graft correctly inside the eye, which requires experience. Graft detachment is more common than with some thicker grafts, and rebubbling may be needed.
Complications include partial or total graft detachment, primary graft failure, endothelial cell loss, pupillary block, raised intraocular pressure, and rare rejection episodes. Despite these risks, DMEK has become a leading choice for suitable patients with endothelial disease.
Epithelial Keratoplasty and Limbal Stem Cell Transplantation
Epithelial keratoplasty is different from PK, DALK, DSEK, or DMEK because it focuses on the ocular surface rather than the deeper corneal layers. The corneal epithelium is the outermost layer of the cornea. It renews constantly and depends on stem cells located at the limbus, the border between the cornea and the white part of the eye.
When limbal stem cells are damaged, the cornea loses its ability to maintain a healthy epithelial surface. This condition is called limbal stem cell deficiency, or LSCD. It may occur after chemical burns, thermal burns, Stevens-Johnson syndrome, ocular cicatricial pemphigoid, severe infection, multiple surgeries, or long-term contact lens-related damage.
In LSCD, the cornea may become covered by conjunctival tissue, blood vessels, and unstable epithelium. Patients can suffer from pain, redness, recurrent epithelial defects, scarring, and severe visual loss. In these cases, a standard corneal transplant alone may fail because the surface cannot heal properly. The ocular surface must first be reconstructed.
Limbal stem cell transplantation aims to replace absent or damaged limbal stem cells so that the cornea can regenerate a stable epithelium. This can be done using tissue from the patient’s healthy eye, from a living related donor, or from cadaveric donor tissue.
Autologous limbal transplantation is used when only one eye is affected and the other eye has a healthy limbus. Allogeneic limbal transplantation is used when both eyes are affected, but it usually requires systemic immunosuppression to reduce rejection risk.
CLET
Cultivated limbal epithelial transplantation, known as CLET, involves taking a small limbal biopsy and expanding the epithelial cells in a laboratory before transplanting them onto the ocular surface. Simple limbal epithelial transplantation, or SLET, uses a small limbal biopsy from the healthy eye, divides it into small pieces, and places them on an amniotic membrane scaffold over the diseased cornea. SLET was first described for treating LSCD and is designed to restore the ocular surface and corneal epithelium.
The advantage of epithelial and limbal transplantation is that it treats the foundation of ocular surface disease. It can restore epithelial healing, reduce pain, decrease vascularization, and prepare the eye for later optical keratoplasty if needed. However, outcomes depend heavily on controlling inflammation, eyelid disease, tear film problems, and autoimmune activity.
Complications include persistent epithelial defects, infection, recurrence of LSCD, graft failure, rejection in allogeneic cases, corneal vascularization, and scarring.
Epikeratoplasty
Epikeratoplasty is an older form of lamellar corneal surgery. In this procedure, donor tissue is placed on the anterior surface of the cornea rather than replacing full-thickness tissue. Historically, it was used for keratoconus, aphakia, and some pediatric corneal problems.
Although epikeratoplasty is much less common today, it remains part of the history of keratoplasty. It showed that corneal surgery did not always have to involve full-thickness transplantation. However, visual outcomes were often limited by interface haze, irregular healing, and induced astigmatism. For most modern indications, it has been replaced by more precise procedures such as DALK and modern endothelial keratoplasty.
summary table
| Type of keratoplasty | Layers replaced | Indications | Advantages | disadvantages | Possible comlications |
| PK | Full corneal thickness | Deep scars, perforation, trauma, advanced keratoconus, failed grafts | Treats complex full-thickness disease | Slow recovery, high astigmatism, open-sky surgery | Rejection, infection, glaucoma, cataract, wound rupture, graft failure |
| DALK | Anterior cornea and stroma, preserving endothelium | Keratoconus, stromal scars, stromal dystrophies | Lower endothelial rejection risk, preserves host endothelium | Technically difficult, possible interface haze | Descemet perforation, double anterior chamber, astigmatism, suture problems |
| DSEK | Endothelium, Descemet membrane, posterior stroma | Fuchs dystrophy, bullous keratopathy, endothelial failure | Faster recovery than PK, smaller incision | Interface may limit vision | Graft detachment, rejection, glaucoma, endothelial loss |
| DSAEK | Same as DSEK, with automated donor preparation | Endothelial disease, complex eyes | More reproducible graft preparation, easier than DMEK | Less optically pure than DMEK | Detachment, hyperopic shift, rejection, graft failure |
| DMEK | Descemet membrane and endothelium only | Fuchs dystrophy, isolated endothelial failure | Best anatomical replacement, excellent vision, low rejection risk | Technically demanding, delicate tissue | Graft detachment, rebubbling, pupillary block, primary graft failure |
| Epithelial / limbal keratoplasty | Corneal epithelium and limbal stem cells | Limbal stem cell deficiency, chemical burns, ocular surface failure | Restores ocular surface, improves healing | May need immunosuppression, depends on surface health | Rejection, persistent epithelial defect, infection, recurrence |
| Epikeratoplasty | Surface donor lenticule | Historical use in keratoconus or aphakia | Extraocular approach | Limited modern use, weaker visual outcomes | /Interface haze, scarring, irregular astigmatism |










Surgical Options in Modern Corneal Transplantation
The choice of corneal transplant surgery depends largely on the affected corneal layer, the severity of the disease, and the condition of the host endothelium. Penetrating Keratoplasty remains an important option for advanced corneal scarring, severe trauma, large perforations, and complex corneal diseases involving all layers of the cornea. Although PKP provides excellent visual rehabilitation in many patients, it is associated with prolonged healing, higher postoperative astigmatism, and a greater risk of endothelial rejection. Despite these limitations, PKP continues to play a major role in cases where lamellar techniques are not technically feasible.
Lamellar keratoplasty techniques have significantly changed the field of corneal transplantation. Deep Anterior Lamellar Keratoplasty is now preferred in stromal diseases with healthy host endothelium, such as keratoconus and superficial stromal dystrophies. By preserving the patient’s own endothelial cells, DALK reduces the risk of endothelial rejection and improves long-term graft survival. In contrast, endothelial disorders such as Fuchs Endothelial Corneal Dystrophy and pseudophakic bullous keratopathy are better managed using endothelial keratoplasty techniques. Descemet Stripping Automated Endothelial Keratoplasty offers relatively easier surgical handling and faster recovery compared with PKP, while Descemet Membrane Endothelial Keratoplasty provides superior visual quality and lower rejection rates due to selective transplantation of Descemet membrane and endothelial cells alone. The continuous evolution of these procedures has shifted modern corneal surgery toward more selective and tissue-preserving approaches.
Conclusion
Corneal transplantation continues to evolve rapidly with the development of advanced lamellar and endothelial keratoplasty techniques. Modern surgical approaches now allow ophthalmic surgeons to selectively replace diseased corneal layers while preserving healthy tissue whenever possible. This transition has improved visual outcomes, accelerated postoperative recovery, and reduced the incidence of graft rejection compared with traditional full-thickness transplantation.
Nevertheless, successful corneal graft surgery still depends on careful patient selection, meticulous surgical technique, and close postoperative monitoring. Early recognition of graft rejection, endothelial failure, elevated intraocular pressure, and infectious complications remains essential for long-term graft survival. As surgical technology, donor tissue preparation, and regenerative therapies continue to progress, the future of corneal transplantation is expected to become even more precise, minimally invasive, and biologically optimized for patients with complex corneal disease.