

Prof. Khaled al Zubi lecture, commentary Prof. Khalil Al-Salem
Diabetic macular oedema (DME) remains one of the leading causes of visual impairment in patients with diabetic retinopathy, and although anti-VEGF agents are considered the first-line therapy, not all patients respond adequately to them. As clinical experience has shown, a significant proportion of eyes exhibit persistent oedema or only partial anatomical improvement even after multiple injections. Consequently, identifying early predictors of anti-VEGF resistance has become increasingly important, as it allows ophthalmologists to intervene more effectively. In this context, the multicentric study on biomarkers associated with switching to dexamethasone (DEX) implant provides valuable real-world evidence that bridges the gap between theoretical knowledge and daily clinical decision-making. OCT-based biomarkers
{kind=link}
{kind=link}
OCT-based biomarkers, in Diabetic macular oedema
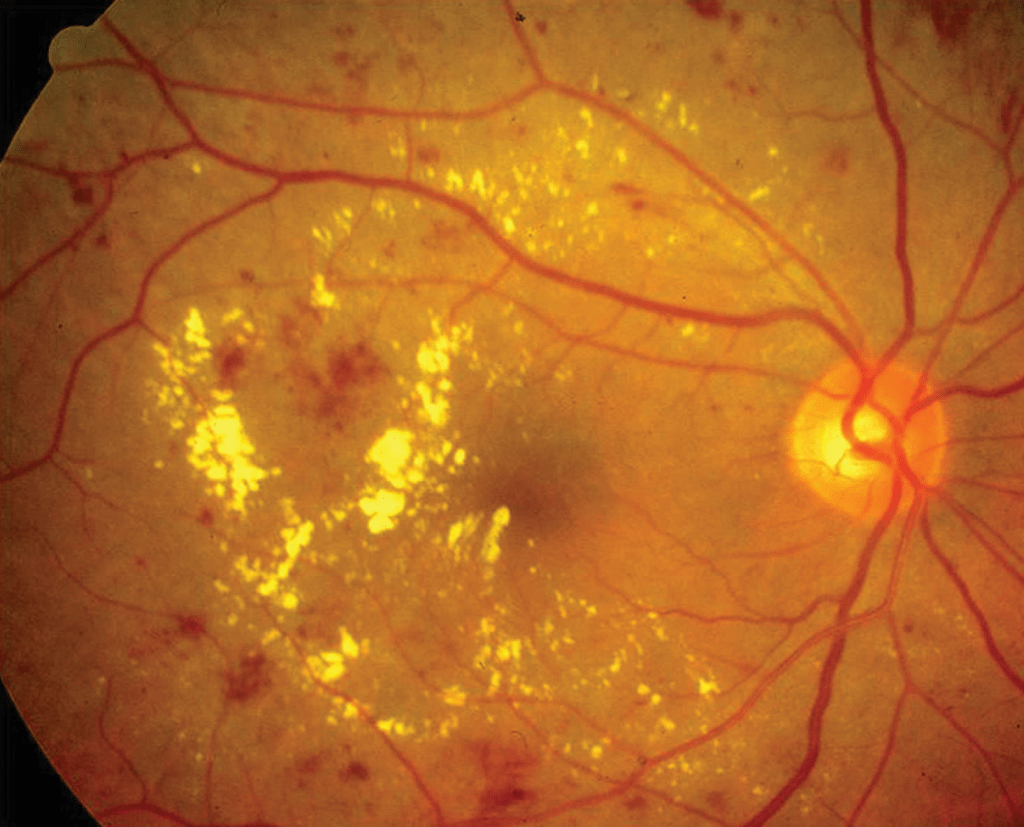
The authors examined a broad range of clinical and imaging characteristics that might influence treatment outcomes. As the analysis progressed, several OCT-based biomarkers emerged as strongly associated with the need to switch therapy. For instance, persistent intraretinal fluid was one of the most consistent signs of poor anti-VEGF response, and this finding aligns with previous literature suggesting that fluid of inflammatory or chronic nature often responds better to corticosteroids. Furthermore, the presence of disorganization of the retinal inner layers (DRIL) added another layer of predictive value, implying that structural damage may limit the functional recovery achievable with anti-VEGF agents alone.
In addition to DRIL, hyper-reflective foci and increased central retinal thickness were repeatedly observed in eyes that ultimately transitioned to DEX. These features may reflect underlying inflammation, lipid migration, or chronic Diabetic macular oedema patterns that tend to respond more favorably to steroid therapy. As the study moved toward evaluating therapeutic outcomes after switching, it became evident that many patients achieved meaningful anatomical improvement once DEX was introduced, which further emphasizes the distinct mechanisms of action between steroids and anti-VEGF therapies.

Ultimately, by combining imaging biomarkers, clinical presentation, and real-world treatment responses. The study provides a coherent framework that supports more personalized management of Diabetic macular oedema. Through the integration of these findings into clinical practice. Ophthalmologists can more confidently identify patients who are unlikely to benefit from prolonged anti-VEGF therapy. Thereby facilitating earlier and more effective use of dexamethasone implants. This transitional approach not only optimizes anatomical results but also enhances the overall quality of patient care.
Biomarkers Switching to Dexamethasone Implant in Diabetic Macular Oedema
Patient Population
Real-world multicentric cohort
Patients with Diabetic macular oedema initially treated with anti-VEGF
Some showing persistent or suboptimal response
Baseline Evaluation & Biomarkers
- Persistent intraretinal fluid (IRF)
- Disorganization of the retinal inner layers (DRIL)
- Hyper-reflective foci (HRF)
- Increased central retinal thickness (CRT)
- Chronic or long-standing oedema
- Inflammatory OCT phenotype
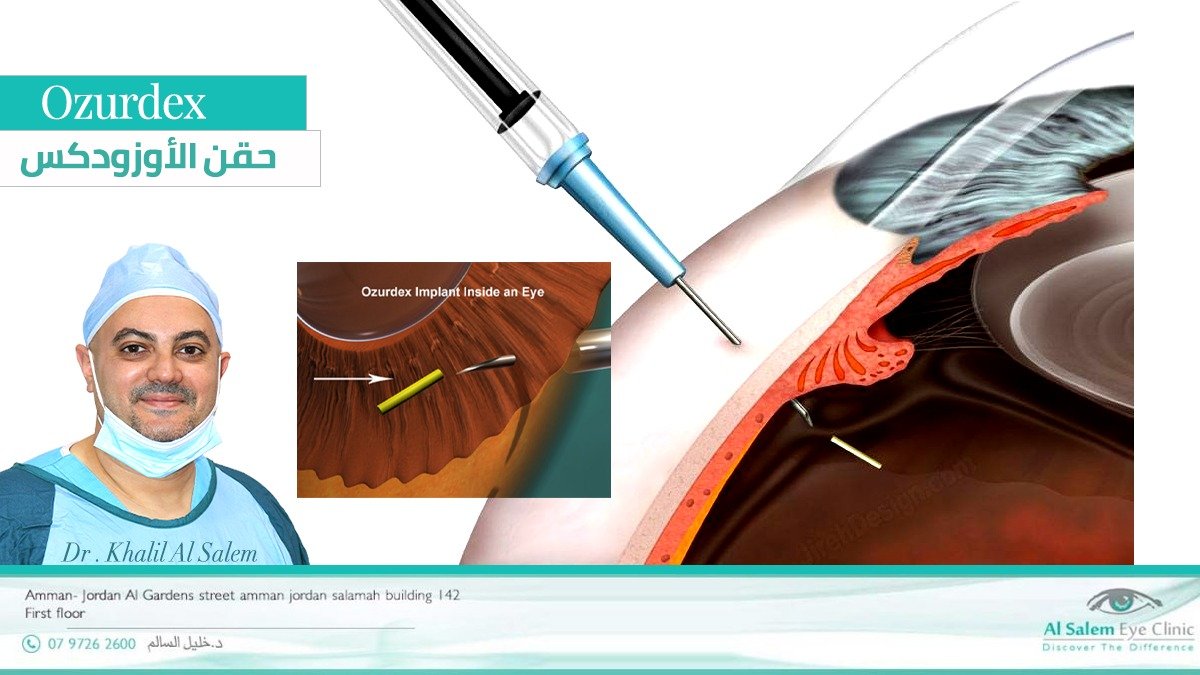
Dexamethasone Implant Therapy (Fourth Panel)
Key Effects diabetic retinopathy:
- Anti-inflammatory action
- Reduction of retinal edema
- Stabilization of retinal layers
Take-Home Message
“Specific OCT biomarkers can predict early anti-VEGF non-response. In addition, it guides timely switch to dexamethasone implants. Improving outcomes in real-world DME management.”